By Frangiska Mylona,
Asthma is a heterogenous disease that affects both adults and children. It is usually characterized by chronic airway inflammation and expiratory airflow obstruction.
This means that the air passages in the lung becomes narrowed, called bronchoconstriction. In this case, it is reversible and produces symptoms of shortness of breath, wheezing sounds, chest tightness, and cough. These symptoms vary over time and intensity and mostly occur at night, early in the morning, or during exercise. In some patients, the result can be airway remodeling with smooth muscle hyperplasia, and hypertrophy of the bronchial glands that add an irreversible component to the obstruction.
Epidemiologically, there has been a significant increase in asthma incidence over the past 40 to 50 years in the Western world. It was recently announced that its prevalence also starts growing in low-income countries as well as in ethnic groups where the incidence was previously low. There are two ideas that justify these concepts.
Firstly, industrialized environments produce many air pollutants that cause allergies. Secondly, there is the hygiene hypothesis stating that city life tends to limit the exposure of young children to some antigens like microbial ones, whereas if they were exposed to them, the incidence of some allergic and autoimmune diseases would have decreased.
As it was previously stated, asthma affects older people and young children. It is evident that asthma is more prevalent in children of color than in Caucasian children.
Asthma can be categorized depending on its clinical phenotypes and pathogenic mechanisms. For instance, there are:
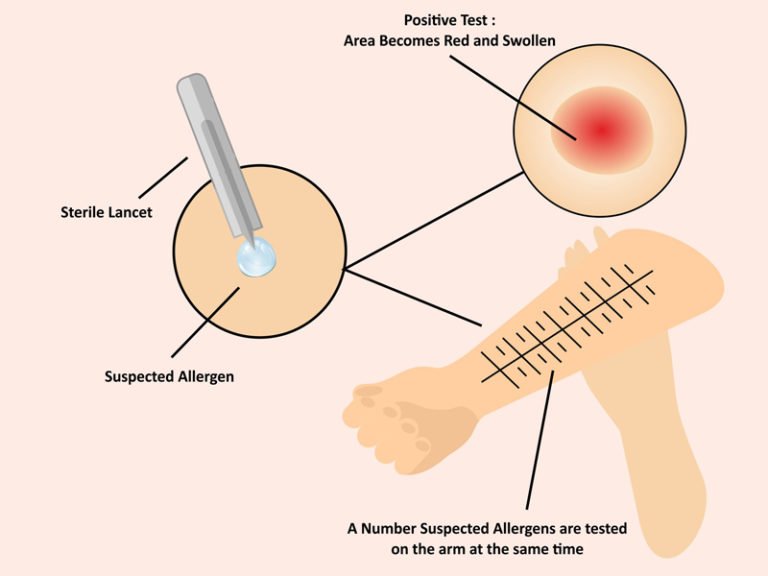
- Atopic Asthma: This is a classic example of asthma triggered by environmental allergens that initiate a hypersensitivity reaction mediated by IgE-antibodies. These antibodies cause allergic reactions and inflammation. This type of asthma starts in childhood from environmental triggers which can be substances like dust, pollen, cockroaches, or even food. These substances irritate the organism along with environmental co-factors such as respiratory viral infections. In this type, patients often have a positive family history of asthma. This leads to the statement that there is a genetic component that contributes to susceptibility to develop this disease. Examples are polymorphisms in genes encoding cytokines like IL-3 and more. The diagnosis is based on high total serum of the IgE- antibodies or by tests proving evidence of allergen sensitization. In atopic asthma, the key inflammatory cells are the eosinophils. Moreover, when a skin test is performed with an offending agent there is an immediate reaction.
- Non-atopic asthma: Individuals suffering from this type have no evidence of allergen sensitization nor a positive skin-test result. Also, it may or may not be a positive family history regarding asthma. The triggers are commonly some viruses like the rhinovirus or the parainfluenza virus as well as inhaled air pollutants such as tobacco, smoke, ozone, and nitric oxide.
- Drug-induced asthma: It is known that several pharmacological agents can provoke asthma. Although it is uncommon, some patients with recurrent rhinitis and nasal polyps may present with aspirin-sensitive asthma. They are also sensitive to other non-steroidal anti-inflammatory medications. The pathogenicity of this mechanism ultimately results in the rapid decrease of prostaglandin E2 which normally inhibits enzymes responsible for the production of some inflammatory mediators.
- Occupational asthma: It is caused by working with substances like fumes (plastics or epoxy resins), gases, chemicals like formaldehyde, and dust such as wood ducts, cotton ducts, and platinum. After repeated exposure to these chemicals, even a small amount of these substances can initiate an asthma attack.
It is a rare phenomenon to suffer from an acute severe asthma attack that can be fatal and it is usually seen in patients with a long history of asthma. A classic asthma attack can last up to several hours, while an acute severe asthma attack can last for days, or even weeks, with paroxysms that can obstruct airflow to the point of death.
Interestingly, not only the environment and genetics are attributed to asthma incidence but also hormones can increase asthma attacks. For example; the female sex hormones may regulate abnormally the β2-adrenergic system which can lead to premenstrual asthma. In addition, emotional factors can trigger specific pathways (such as the vagal pathway), which induce bronchospasm.
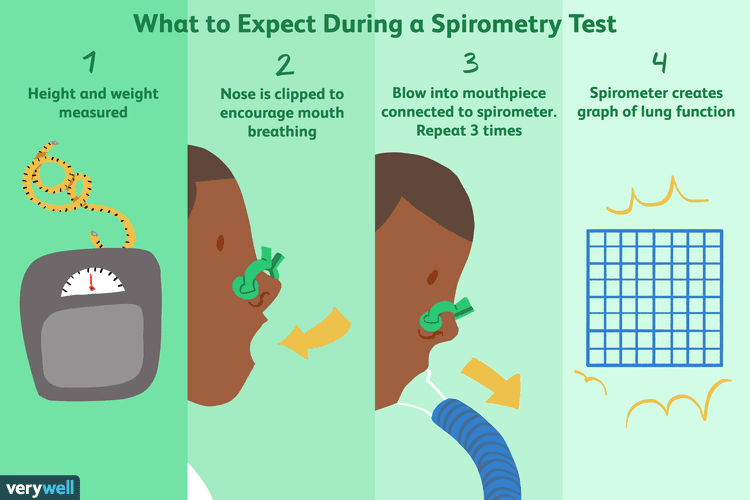
Generally, the diagnosis is based on a detailed medical history, physical examination, laboratory findings (including the eosinophils for patients with atopic asthma), and pulmonary function tests like spirometry. By using spirometry, the airflow obstruction can be demonstrated and problems with exhalation can be identified. Based on its findings, asthma patients (over or equal to twelve years of age) can be classified into four severity levels enabling more effective therapy treatment and lung function monitoring.
The categorization system, starts from intermittent, to mild, moderate, and severe, with profound limitations on the patient’s normal activity.
As mentioned earlier, treatment depends on asthma severity. There are many ways to treat asthma attacks. At first, there are pharmacological therapies including inhaled drugs such as bronchodilators, glucocorticoids, corticosteroids, and leukotriene antagonists. Some novel biologic therapies such as IL-5 blocking antibodies exist for difficult-to-treat asthma patients in adolescents and adults. In cases of acute asthma attacks, some quick-relief medications are used including short-acting β2-adrenergic agonists that relax the bronchial smooth muscle and provide quick relief of symptoms usually in 30 minutes.
Moreover, there are preventive non-pharmacological measures to control factors that contribute to asthma attacks. These include educating the family and the patient about avoiding exposure to allergens and irritants. They also include disinfecting their residences from dust and insects regularly. In addition, they should remember that factors like nasal polyps, aspirin sensitivity, and gastroesophageal reflux can affect asthma. It is recommended to perform an annual influenza vaccine for patients with persistent asthma.
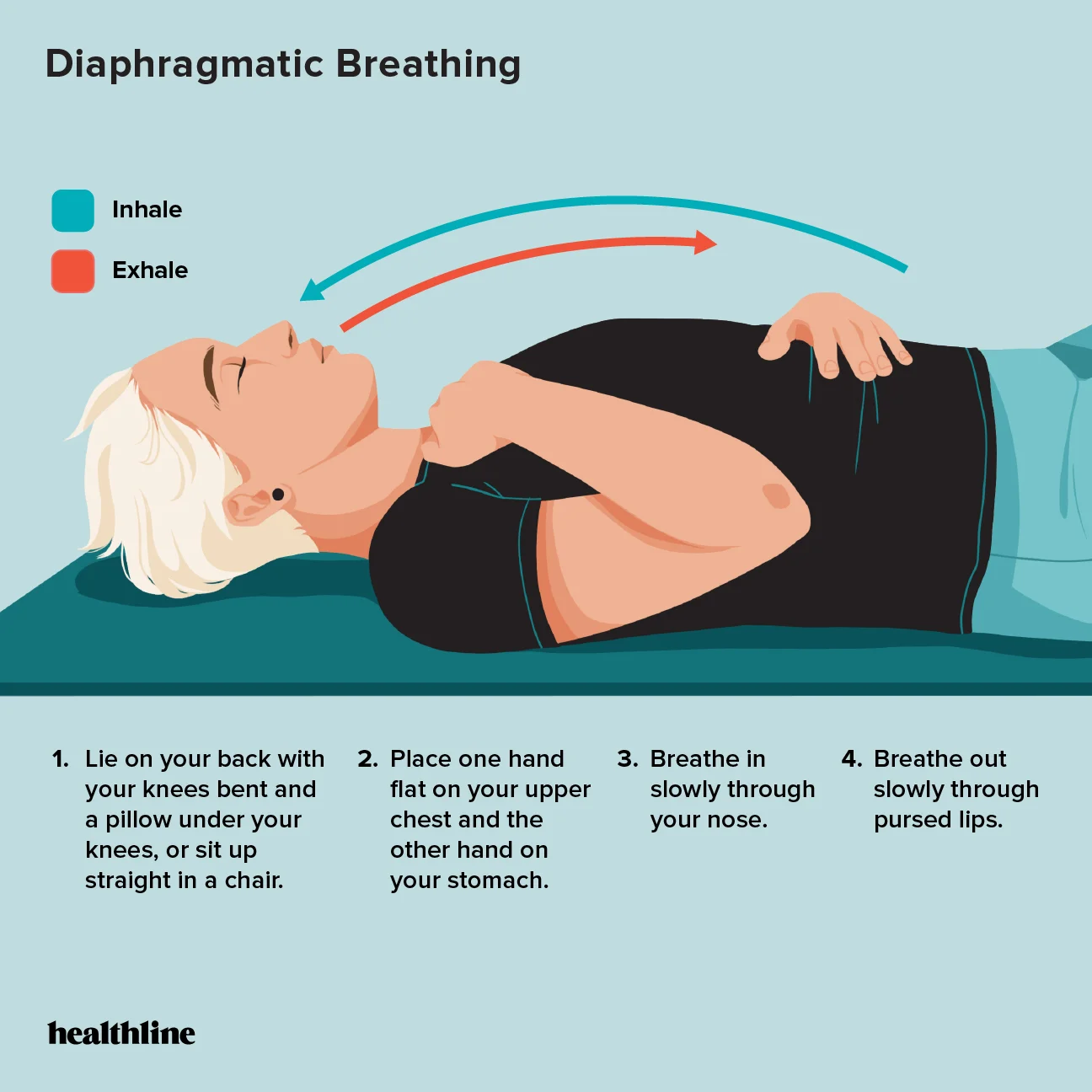
Other non-pharmacologic methods include relaxing techniques, controlled breathing, and reducing anxiety and panic that aggravate breathing difficulties. Additionally, improving sleep quality as well as dietary lifestyle are significant measures in preventing asthma attacks. Also, children should learn to be independent regarding their symptom control as well as to develop a positive mindset even though they face the difficulties of the disease.
Patients suffering from asthma are usually asymptomatic in between attacks, so when attacks occur, many patients find it very difficult to maintain a productive life. Therefore, patient behavior is crucial to effectively controlling asthma. Asthma management requires patients to actively engage in self-management behaviors to adhere to therapy regimens. When patients adhere to these multiple recommendations it is logical that asthma can be controlled effectively. However, many studies have found that poor adherence to asthma self-management is very common, and significant contributors to inadequately-controlled asthma are either disengagement in measures that reduce asthma triggers such as appropriate cleaning or not regularly performing insect and dust disinfection. Also, since tobacco and smoke are one of the environmental triggers of asthma, it is advised for patients to quit smoking or disengage themselves from places with tobacco, however many of them continue to be exposed.
In conclusion, asthma is a chronic condition that needs to be controlled and regulated for the patient to continue living a full life. Even though sometimes, it can be restrictive, by keeping a positive attitude towards it and by being compliant with the pharmacological treatment as well as by adopting a healthy lifestyle, the patients will have a normal life expectancy as well as they will be able to engage to the normal everyday activities.
References
- Robbins & Cotran, Pathology of diseases, 10th edition by Kumar Abbas Aster.
- Porth’s Essential of Pathophysiology; 5th edition by Tommie L. Norris and contributing author; Rupa Lalchandani Tuan, Ph.D.