By Frangiska Mylona,
At least everyone, once in their lifetime, has experienced a nosebleed. Either by accidentally scratching their nose or by getting hit, or in cases of increased blood pressure. Nevertheless, it is a common phenomenon that in some circumstances may indicate a pathological condition.
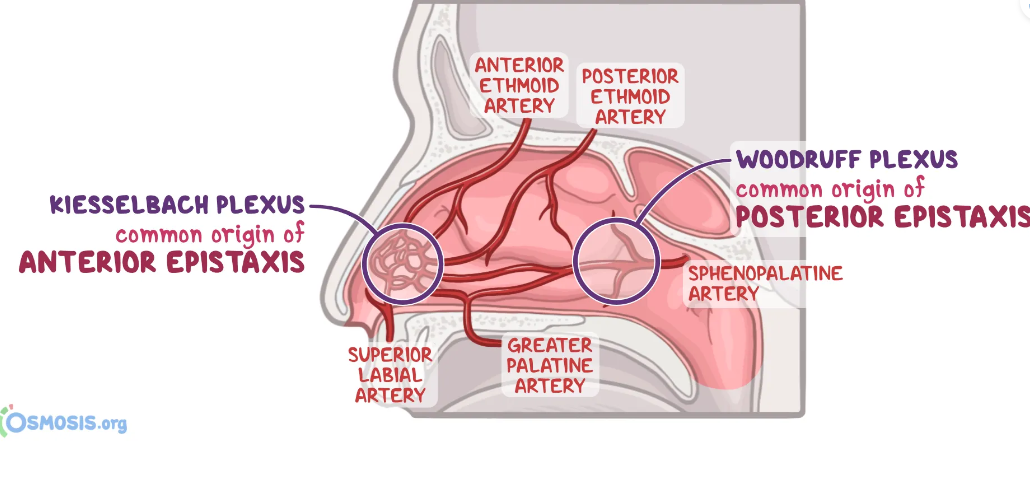
Nosebleed or epistaxis is divided into two big categories depending on which arteries are affected. The anterior epistaxis is common in children due to minor trauma, involving a tear in the Kisselbach’s plexus (known otherwise as the Little’s area) which supplies the anterior part of the nasal cavity. The Kisselbach’s area is the place of the anastomosis of five arteries which are branches of the external and internal carotid arteries, respectively.
The posterior epistaxis is a more urgent phenomenon, manifesting with heavy bleeding, indicating a tear in the sphenopalatine artery, which supplies the posterior part of the nasal cavity. Its etiology can be an indicator of a serious condition, since it is associated with hypertension, telangiectasia, hemophilia or tumors. Additionally, it can be the result of the adverse effects of anticoagulants and it is more common in elderly patients.
The main key to treat an epistaxis is to calm the patient and to ensure that their airways are clear and that breathing is preserved. The most common approach is to stop it by leaning forward (not backwards, since blood-swallowing should be avoided) and pressing both sides of the nose with the index and middle finger until the bleeding stops. For nosebleeds that are unsuccessfully ceased by this maneuver, there are interventional methods like anterior or posterior nasal packing, cauterization with local anesthetics and, for even more serious epistaxis, ligation of the responsible arteries.
The juvenile nasopharyngeal angiofibroma is a rare vascular benign tumor found in the nasal cavity, which, even though benign, is very locally aggressive. Its usual location is in the roof of the nasal cavity at the superior margin of the sphenopalatine foramen and it can extend till the pterygopalatine fossa, nasopharynx, sphenoid and ethmoidal sinuses or in the middle cranial fossa.
The mean epidemiological age of patients is around their teenage to early adolescent years between the ages of 15 to 25, affecting almost exclusively males. The main clinical symptoms include nasal obstruction with recurrent massive and heavy epistaxis with possible anosmia and frog face deformity.
The most fascinating part about this tumor is that biopsy is contraindicated, even though in oncology, biopsy is considered one of the most important elements for correct diagnosis. The etiology for this contraindication lies solely on the highly vascular nature of the tumor, and biopsy could induce an uncontrollable hemorrhage. Instead, the diagnosis is conducted via imaging modalities and the clinical presentation.
On the CT scan, the tumor can be seen as a multilobulated structure that is enhanced if contrast is injected. It can also induce bone remodeling and it is possible to directly invade the bone. MRI is performed in order to assess the relation of the tumor with important and delicate structures like the internal carotid artery or the pituitary gland. Another approach involves carotid arteriography for the visualization of the tumor’s blood supply.
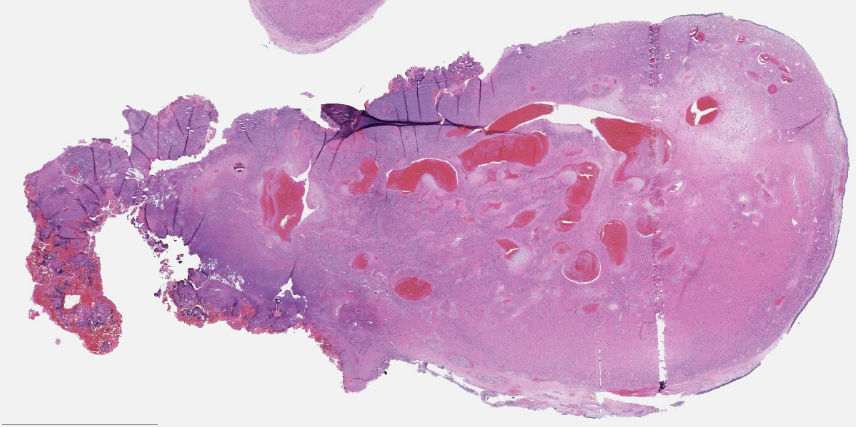
Macroscopically, the lesion is firm, rubbery, grayish, purple or red with possible ulcerations, broadly attached to the wall of the nasopharynx. Microscopically, it includes spindle-shaped cells, lymphocytes and plasma cells. The small or medium-sized vessels appear malformed with incomplete elastic laminae.
Another interesting fact is that it is an androgen-dependent tumor that can respond well to hormonal treatment. Other therapeutic approaches involve preoperative embolization or internal maxillary artery ligation and subsequent surgical removal (which can be endoscopic or open) along with radiotherapy to shrink the tumor.
In conclusion, juvenile nasopharyngeal angiofibromas present with frequent, heavy epistaxis in adolescent boys along with the feeling of smell loss and frog face deformity. Biopsy, in this case, is contraindicated and the diagnosis is done with the use of imaging methods and symptomatology. Lastly, it is an androgen sensitive tumor, therefore it can respond well to hormonal treatment.
References
- Lorne H. Blackbourne. “Surgical Recall”. FACS. 9th Edition.
- Virginia A.Livolsi, Maria J.Merino, John S.J.Brooks, Scott H.Saul, John E. Tomaszewski. “Pathology”. The National Medical Series for Independent Study, 3rd Edition.
- Juvenile Nasopharyngeal Angiofibroma; Site of Origin, Staging, Clinical Features, Clinical examination, Diagnosis, Treatment. Prepladder. Available here