By Frangiska Mylona,
A medical institution like a hospital needs to organize its patients based on the severity of their problems. As it is logical, patients who are on the verge of dying should be given more urgent attention than those who are in discomfort or need a quick checkup. The practice of prioritizing medical care is called triage.
The triage practice is not a “revolutionary” organization system because it has a historical background. The term “triage” derives from the French verb “trier” which means to sort. Napoleon, this clever French military leader, developed the triage system to serve as a battlefield clearing hospital for wounded soldiers. As this method developed, it became more complex with more variants, for instance in World War I and II, triage was the procedure that determined which soldiers would be able to return to the battlefield, while in the Korean War that was connected with “doing the greatest good for the greatest number of wounded and injured”. Today, this system is not only used in hospitals for better categorization but is even applied in mass causality incidents for determining the severity of the injured. Consequently, the triage concept is separated into the following categories: ED triage, inpatient (ICU) triage, incident (multi-casualty) triage, military (battlefield) triage, and disaster (mass casualty) triage. This article will mostly focus on the triage system that is used in the emergency departments of hospitals.
To be able to understand the meaning of triage, three conditions must be described in an attempt to define its use in the medical field;
1) Consider the scenario in which there are so many resources and medical staff that all patients can be addressed and treated simultaneously. This scenario is by far the best-case scenario, but it would not be a need for a triage system! On the other hand, imagine a hospital or a healthcare institution where no healthcare resources are available, and consequently, the triage system is pointless. Therefore, for the triage system to be able to get established, there must be a slight scarcity of medical resources so that prioritization has meaning.
2) A healthcare worker assesses each patient’s medical situation, usually based on a brief examination.
3) The healthcare worker uses a plan that is based on an algorithm or a set of criteria to determine the treatment priority for each patient. As a result, triage is distinguished from other purely arbitrary organization systems regarding the distribution of health care resources.
All of the aforementioned triage types follow these principles, even if they have some differences from each other.
Regarding the triage system, there is no universal model. There are general variations of this system around the world for example the Australasian triage system, the European triage system, the North American triage system, the Asian triage system, the African triage system, and also the triage system can be divided regarding the age of the patient like the pediatric triage system. A modern triage system consists of a comprehensive apparatus for categorizing patients according to vital sign parameters such as level of consciousness, respiratory rate, heart rate, blood pressure, oxygen saturation, and body temperature. All of these are accommodated by the clinical image of the patient.
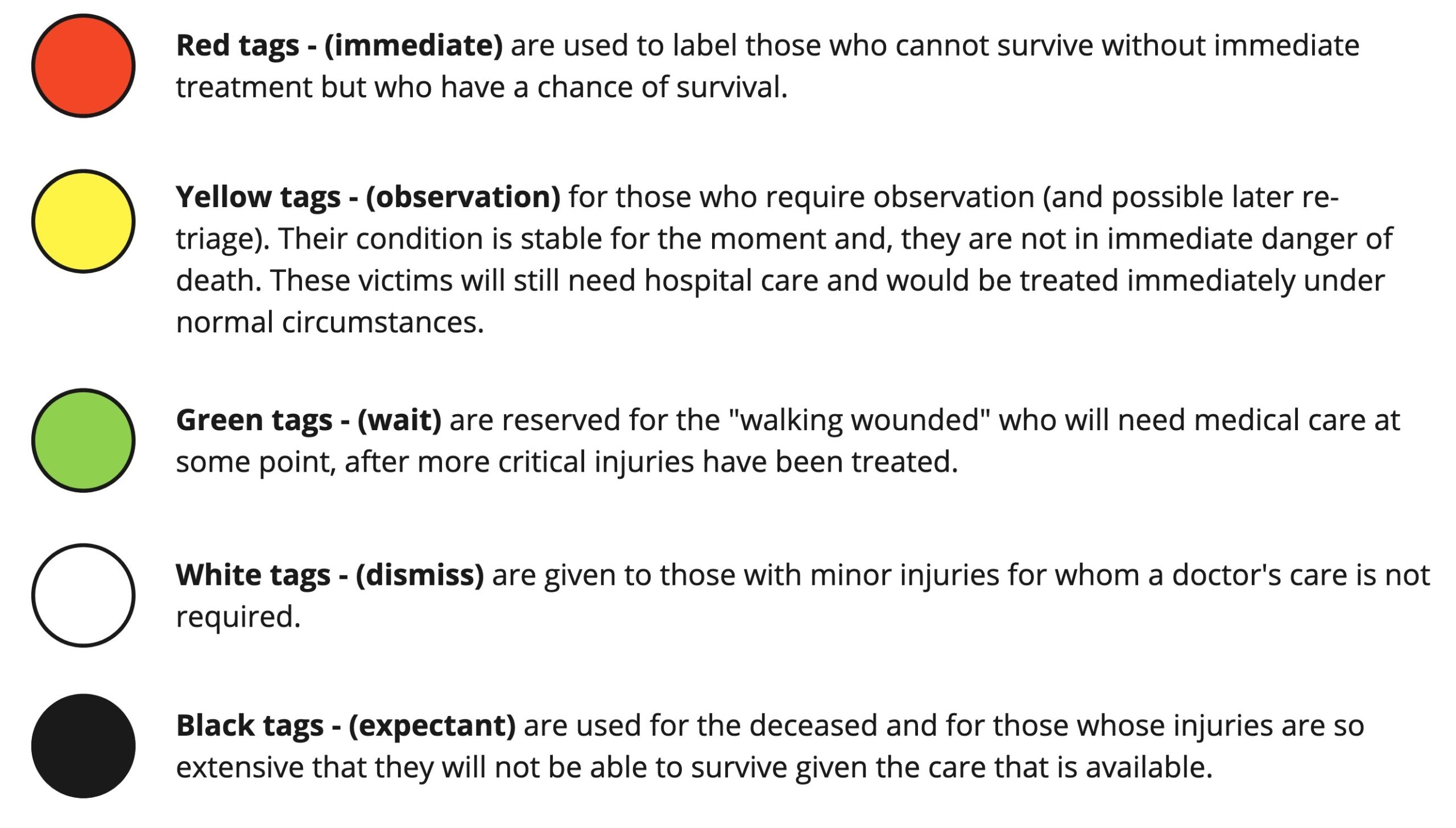
More specifically, the modern triage system categorizes patients based on a “color system” including five levels with five different colors;
● Death expectancy – Black; this level includes very severely injured or impaired patients f.e. severely burned patients, patients in cardiac arrest, patients in septic shock, and patients with severe head trauma… In these cases, the palliative approach usually focuses on how to treat and alleviate pain.
● Immediate – Red; at this level, some patients require immediate care and stabilization including cardiac resuscitation, ventilation, surgery, or even transportation to more advanced facilities after they have been stabilized like patients with severe hemorrhage, amputations, heart attacks, or even patients with severe anaphylaxis.
● Very urgent – Yellow (in some countries it might be orange); at this level, there are patients with severe injuries but with stable vital signs. These patients require constant observation and rapid treatment but there is a high chance that they will survive. Examples are patients with severe fractures and dislocations and minor amputations…
●Standard – Green; patients are in this category if they have suffered a minor injury that needs treatment and they will be discharged soon. Patients may suffer from sprains, abrasions, and minor lacerations …
● Non-urgent – White; patients in this category have a few minor complaints or need a quick check-up. Usually, patients wait much longer in the waiting rooms since they do not suffer from something urgent or serious.
The color variation in each country varies, as was mentioned previously. For example, in Germany, the blue color signifies that the patient has a very low chance of survival meaning that it is an “intermixed” signal between the red and black colors. The presence of the orange color that is between the red and yellow colors on the chart indicates that the patient has an urgent need for treatment.
A second interesting approach to the medical triage system is the assessment of victims in the multi-casualty triage system. The approach is called START. START stands for Simple Triage And Rapid Assessment and it is based on algorithms that quickly place victims on the appropriate scale in the triage system. The multi-casualty triage system also uses the SALT method standing for Sort-Assess-Lifesaving Interventions-Treatment/Triage. One of their major differences is the ”gray” category that is included in the SALT system. Patients who are categorized as “gray” are the “expected” victims who are still alive but have massive injuries or are likely to die shortly. In addition, some patients may require primary or secondary care after they have undergone the START system which is offered by the SALT system.
Ethical problems that could arise when the medical triage system is applied, is the thought that this system ”chooses”, in a way, the patients that will die (patients in the color ”black”) from the immediate urgent patients that might have a higher chance of surviving (patients in the color ”red”). It should be understood that this is a misconception. The priority of the medical triage system is not to determine whether patients will die, but rather to determine which patients will survive. In this case, death for some of the severely impaired is considered a circumstance, but it is not the goal of the triage system. After all, medicine aims to preserve life and treat people who are in need as effectively as possible. In addition, two values are preserved in the healthcare profession and thus in the triage system; the principle of medical necessity and the principle of priority.
As it was mentioned earlier, medical triage systems exist because the number of medical supplies and the number of medical personnel are less than the number of patients that should be treated every day. In other words, it makes sense that if medical supplies had to be spent, the most impaired patients would be selected first meaning that the values of priority and necessity are interchangeable concepts in the medical triage system. In everyday medicine, the same logic is applied, especially in situations involving a multi-casualty incident, when it is necessary to save as many people as possible.
In conclusion, medical triage has been embedded in historical and modern times as a system that encompasses the values of help, care, and treatment and it strives to save as many lives as possible. Although it is wrapped around the tragedy of death, it prioritizes all medical resources in order to save every patient that can and will survive.
References
- Douvika, E. (Elena). (2022). Comparative approach of triage’s legal regulation. Bioethica, 8(2), 65–84. Available here
- Sharon E. Mace MD, Thom A. Mayer MD, in Pediatric Emergency Medicine, 2008.
- Triage in Medicine, Part I: Concept, History, and Types Kenneth V. Iserson, MD, MBA John C. Moskop, PhD